
The Trigeminocervical Complex (TCC) refers to the relationship between the upper neck, TMJ (Jaw), and trigeminal nerve, which can be associated with a wide range of conditions that affect the neck, face, and head.
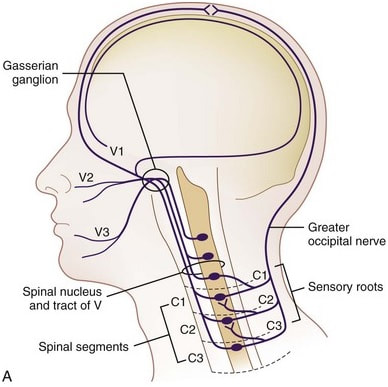
The first two joints in the neck are uniquely shaped compared to the rest of the cervical spine. They demonstrate a different set of movement patterns, have their own special muscles to produce those movements, and enjoy special connections to the nervous system that the rest of the surrounding tissues do not have. In particular, these joints connect to a cluster of nerve tissue that joins a number of areas in the face and skull. The jaw joint also shares a neighbourly relationship with some of this nerve tissue and can be involved in much the same way as the upper neck.
What this means is that pressure, temperature, or other stimulus of these muscle or joint tissues can contribute to the overall signal being sent to our brain and the nerves of our skull and face. In this way, the muscles and joints in the upper neck and jaw can contribute to the average tension headache as well as the more complex association for migraine and other painful conditions involving the face. People who are experiencing headache complaints will also typically demonstrate increased sensitivity in these areas.
At a physiological level, all of our sensation is at some point electrical signals carried by our nerve tissue. The mechanical forces and feelings of the upper neck and jaw can amplify the signal of nearby nerves. If this amount of electrical signal is above a certain threshold in the body, it has the potential to produce feelings of tension, pain, numbness, tingling, pins & needles, tinnitus (ringing in the ears), headache, and more.
If the nerves are particularly irritated, the presentation can include congestion of the sinuses, watering of the eyes, and irritability of the eyelids. Some more unusual symptoms that can be attributed to this area include bulging of the eyes, running sinuses, a sense of fullness in the ears, a feeling of tightness in the throat, and a general flushing of the skin in the neck and face.
Assessment and treatment of conditions that affect the Trigeminocervical Complex and surrounding tissues can often be complex and require multiple perspectives and professionals to develop a satisfactory program. Family Physicians, Specialists such as Ear-Nose-Throat (ENT) Physicians, Audiologists, Neurologists, and Physical therapists often work together to manage all aspects of the presentation.
While not all conditions in this area will have a mechanical relationship, as there are several diseases and medical conditions which can be a root cause as well, it can still be of value to look at conservative and non-invasive medical treatment before moving on to more investigations and tests.
With appropriate management and restoration of the mechanical features in these areas, including hands on treatment and therapeutic exercise prescription, the overall stress on the tissues and nervous system can typically be reduced.
If there are any questions or comments regarding this information, please feel free to comment here or reach out to our office.
-Trent, PT
References
The first two joints in the neck are uniquely shaped compared to the rest of the cervical spine. They demonstrate a different set of movement patterns, have their own special muscles to produce those movements, and enjoy special connections to the nervous system that the rest of the surrounding tissues do not have. In particular, these joints connect to a cluster of nerve tissue that joins a number of areas in the face and skull. The jaw joint also shares a neighbourly relationship with some of this nerve tissue and can be involved in much the same way as the upper neck.
What this means is that pressure, temperature, or other stimulus of these muscle or joint tissues can contribute to the overall signal being sent to our brain and the nerves of our skull and face. In this way, the muscles and joints in the upper neck and jaw can contribute to the average tension headache as well as the more complex association for migraine and other painful conditions involving the face. People who are experiencing headache complaints will also typically demonstrate increased sensitivity in these areas.
At a physiological level, all of our sensation is at some point electrical signals carried by our nerve tissue. The mechanical forces and feelings of the upper neck and jaw can amplify the signal of nearby nerves. If this amount of electrical signal is above a certain threshold in the body, it has the potential to produce feelings of tension, pain, numbness, tingling, pins & needles, tinnitus (ringing in the ears), headache, and more.
If the nerves are particularly irritated, the presentation can include congestion of the sinuses, watering of the eyes, and irritability of the eyelids. Some more unusual symptoms that can be attributed to this area include bulging of the eyes, running sinuses, a sense of fullness in the ears, a feeling of tightness in the throat, and a general flushing of the skin in the neck and face.
Assessment and treatment of conditions that affect the Trigeminocervical Complex and surrounding tissues can often be complex and require multiple perspectives and professionals to develop a satisfactory program. Family Physicians, Specialists such as Ear-Nose-Throat (ENT) Physicians, Audiologists, Neurologists, and Physical therapists often work together to manage all aspects of the presentation.
While not all conditions in this area will have a mechanical relationship, as there are several diseases and medical conditions which can be a root cause as well, it can still be of value to look at conservative and non-invasive medical treatment before moving on to more investigations and tests.
With appropriate management and restoration of the mechanical features in these areas, including hands on treatment and therapeutic exercise prescription, the overall stress on the tissues and nervous system can typically be reduced.
If there are any questions or comments regarding this information, please feel free to comment here or reach out to our office.
-Trent, PT
References
- Pressure pain thresholds over the cranio-cervical region in headache: a systematic review and meta-analysis. Castien et al. The Journal of Headache and Pain (2018) 19:9
- Understanding Cervicogenic Headache. Chua, N., Suijlekom, H., Wilder-Smith, O., Vissers, K. Anesthesiology and pain medicine. Feb 2012.
- Cluster Headache: Epidemiology, Pathophysiology, Clinical Features, and Diagnosis. Wei, D., Ong, J., Goadsby, P. Annals of Indian Academy of Neurology. April 2018.
- Head pain referral during examination of the neck in migraine and tension-type headache. Watson DH., Drummond PD. Headache. Sept 2012.
 RSS Feed
RSS Feed